By: Osteopath Vladimir Levachyov
When it comes to alleviating a headache, in my experience, the pain is routinely either badly treated or poorly controlled.
Headaches are one of the most common problems patients discuss with me in our sessions. The first port of call is a thorough case history in order to identify if the pain is due to a primary or a secondary headache (where the headache is a symptom of a different problem, which needs treating first). Most commonly, headaches seen in clinic are primary, for example migraines, tension headaches, or cervicogenic headaches – which is the subject of this post.
My approach to headaches has been fine-tuned through attending a course on headache management for osteopaths organised by Osteopaths for Progress in Headaches and Migraines (OPHM). I’ve had the pleasure of hearing and participating in lectures given by Helena Bridge, the Headache Clinic Lead at the European School of Osteopathy and a founding member of OPHM; as well as Danny Orchard, a pain specialist and the founder of the Centre for Osteopathic Research and Excellence (CORE). I’ve been fortunate enough to be able to keep in touch with both of them since, particularly Danny, as I volunteer as an osteopath at CORE on a weekly basis.
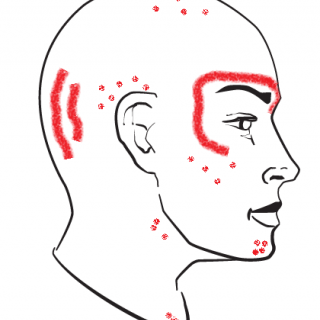
So, what are cervicogenic headaches? Cervicogenic means “coming from the neck” and so cervicogenic headaches arise due to poor neck function. The way in which neck tension can cause headaches is relatively simple; muscles at the base of the skull can become so tight as to crush the nerves that supply feeling/sensation to the skin at the base of the skull, over the temple, as well as the skin over the eyebrow.
Please note my diagram above which depicts the most common referral pattern of a cervicogenic headache. The solid lines represent the most common locations for the pain, whereas the dots show the less common places for the pain to be felt.
Cervicogenic headaches are often eased in the short term by soft tissue techniques (massage, inhibition, stretching, etc) applied to those muscles at the base of the neck, the suboccipital muscles.
Depending on the pattern of dysfunction, spinal manipulation can have a positive effect for some patients. The use of this technique is decided on a case by case basis following a thorough screening for safety. Dry needling (medical acupuncture) techniques can also be very beneficial.
In the medium to long term I investigate the factors resulting in tightness of the suboccipital muscles such a badly set up desk (insufficient screen height, or working on laptops and having to look down for extended periods), as well as other mechanical factors like any tightness between the shoulder blades which can lead to neck overuse or repetitive strain injuries.
Outside of the clinic every headache patient is prescribed a specific and bespoke programme of home exercises that will help to alleviate neck tightness and address any contributing factors.
Our treatment approach is underpinned by scientific clinical evidence on the subject, some choice sources include:
- The Journal of the American Osteopathic Association: Cervicogenic Headache: A Review of Diagnostic and Treatment Strategies.
- International Journal of Osteopathic Medicine: Effectiveness of cervical spine manipulation and prescribed exercise in reduction of cervicogenic headache pain and frequency.
- Cephalgia journal: Evidence for the use of dry needling and physiotherapy in the management of cervicogenic or tension-type headache: a systematic review.